
Case study series
Low back pain - Sciatica
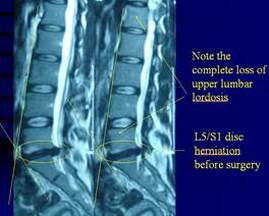
This is an interesting case I would like to share with you and I hope more of such patients could be helped. A 26-year-old otherwise fit and sporty lady gradually developed left buttock/hip pain in May 2009. Symptoms continued to worsen with leg pain and numbness despite intensive medical and physical treatments. She was forced to resign from work in Beijing and return to Hong Kong for surgery.Microdiscectomy (removal of the protruding disc fragment) was performed in October with good result initially but symptoms recurred a month later. She continued to seek conservative treatment, hoping to prevent the second operation suggested. Presentation in March 2010 when I first saw her revealed very much reduced lordosis (the forward/inward S-curve of the low back) in the lower lumbar (low back) and even kyphotic (backward/outward or reverse of the S-curve of the low back) in the upper lumbar spine. Lumbar flexion (forward bending) was severely restricted to 1/5 range with marked leaning of the body to the left. Back turning and backward bend were restricted to 3/4 range. Slump (forward slouch with straight legs) test was positive. Sciatica nerve flexibility was severely restricted with pulling pain. Other specific spine movements were generally stiff more on the left with surrounding soft tissue thickening (scarring).
Clinical presentation suggested recurrent lower lumbar (low back) disc derangement, chronic lumbar dysfunction and facet joint stiffness/thickening with severe neural (nerve) adhesion. The reasons for recurrence must be found to aim appropriate physical treatment and prevention of the second operation. The problem of the very much reduced lumbar lordosis due to chronic lumbar dysfunction as a result of poor posture or previous trauma had never been addressed before or after the operation. Poor specific spine movements as a result of thick and stiffened intervertebral and facet joints had never been restored before and after the operation. Severe scar tissue formation as a result of insufficient rehabilitation (passive & active mobilizations, therapeutic exercises & advice) had led to severe neural (nerve) adhesion. Treatment aim was torestore lumbar (low Back) mobility and alignment to minimize neural adhesion and to prevent future aggravations. Besides the necessary manipulative techniques, the patient’s effort of performing her rehabilitation exercises and awareness of her condition was crucial to her speedy recovery within three month when she could gradually return to her sports.
Clinical presentation suggested recurrent lower lumbar (low back) disc derangement, chronic lumbar dysfunction and facet joint stiffness/thickening with severe neural (nerve) adhesion. The reasons for recurrence must be found to aim appropriate physical treatment and prevention of the second operation. The problem of the very much reduced lumbar lordosis due to chronic lumbar dysfunction as a result of poor posture or previous trauma had never been addressed before or after the operation. Poor specific spine movements as a result of thick and stiffened intervertebral and facet joints had never been restored before and after the operation. Severe scar tissue formation as a result of insufficient rehabilitation (passive & active mobilizations, therapeutic exercises & advice) had led to severe neural (nerve) adhesion. Treatment aim was torestore lumbar (low Back) mobility and alignment to minimize neural adhesion and to prevent future aggravations. Besides the necessary manipulative techniques, the patient’s effort of performing her rehabilitation exercises and awareness of her condition was crucial to her speedy recovery within three month when she could gradually return to her sports.

|
|
Luck LI
Musculoskeletal Physiotherapist
Musculoskeletal Physiotherapist